

The U.S. has fared worse than other countries not because it lacked information or funding but because it failed to learn the lessons of the last outbreaks.
In 2006, the idea that an unknown virus might spill out of some wild animal into humans, achieving person-to-person transmission and causing a global pandemic, seemed a distant prospect to most people. As an engaging science-fiction scare, it ranked somewhere beneath “Alien: Resurrection.” But Ali S. Khan, of the National Center for Zoonotic, Vector-Borne, and Enteric Diseases, was tasked with dreaming that nightmare by daylight.
nczved (pronounced “N. C. Zved,” according to Khan), part of the Centers for Disease Control and Prevention, resided in an unobtrusive gray brick building, behind locked gates and locked doors in the C.D.C.’s compound on Clifton Road, six miles northeast of downtown Atlanta. During a two-day visit that year, I worked my way along the nczved corridors, interviewing scientists who knew all about Ebola viruses (yes, there are more than one) and their lethal cousin Marburg; about West Nile virus in the Bronx and Sin Nombre virus in Arizona; about simian foamy virus in Bali, which is carried by temple monkeys that crawl over tourists, and monkeypox, which reached Illinois in giant Gambian rats sold as pets; about Junin virus in Argentina and Machupo virus in Bolivia; about Lassa virus in West Africa, Nipah virus in Malaysia, Hendra virus in Australia, and rabies everywhere. All these viruses are zoonotic, meaning that they can pass from animals to people. Most of them, once in a human body, cause mayhem. Some of them also transmit well among people, bursting into local outbreaks that may kill hundreds. They are new to science and to human immune systems; they emerge unpredictably and are difficult to treat; and they can be especially dangerous, as reflected in the name of the branch within nczved that studied them—Special Pathogens. For these reasons, some scientists and public-health experts, including Ali Khan, find the viruses an irresistible challenge. “It’s because they keep you on your toes,” he told me. On the second day of my visit, amid the intriguingly gruesome briefings, Khan took me out for sushi.

Khan is a medical doctor by training, an epidemiologist by career, and a man of candid, irreverent jocularity. He was wearing an epauletted uniform sweater; at the time, he was also an officer in the United States Public Health Service, which is organized into ranks, like those in the U.S. Navy. “You’ve heard all the talk from our people,” he said. “Which of these diseases is your favorite?”
My favorite? Ebola is pretty damn interesting, I told him.
“Aaah,” Khan said dismissively. “I like Ebola as much as the next person.” He had done crucial epidemiological work during the 1995 Ebola outbreak in Kikwit, in what was then Zaire, organizing control measures, investigating transmission, tracing the outbreak back to its Patient Zero, risking his life to help end a juggernaut of misery and death. He continued, “But, for my money, sars was the one.”
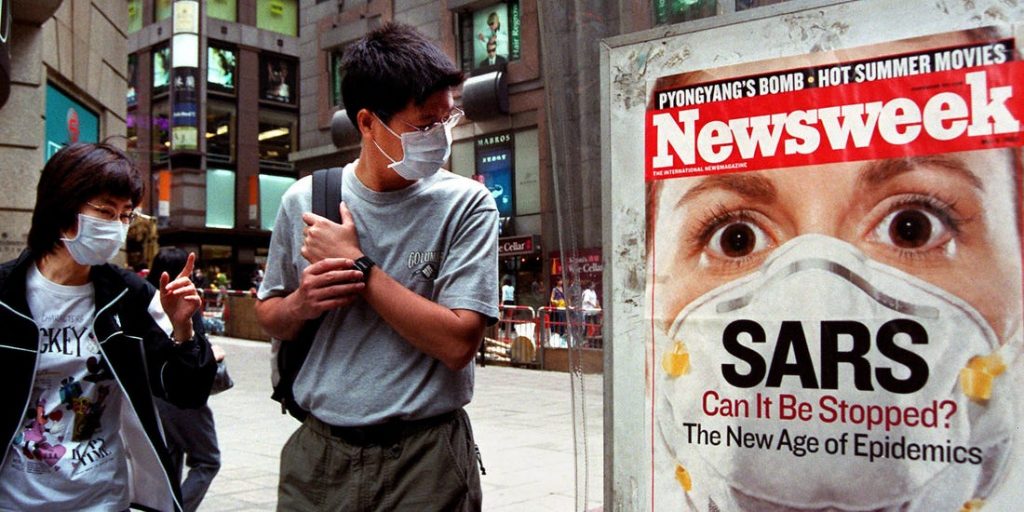
sars? I knew of it only as a bad viral disease that, in 2003, came out of southern China and killed people in Toronto, Singapore, and a few other cities. The acronym stands for “severe acute respiratory syndrome.” It’s an ugly illness that can lead to lethal pneumonia. A little more than eight thousand people were infected, of whom about ten per cent died, and then the outbreak ended. “Why sars?” I asked.

“Because it was so contagious, and so lethal,” he said. “And we were very lucky to stop it.” sars was the bullet that went whistling past humanity’s ear. This was on our lunch break, I had stopped taking notes, and it was fourteen years ago, so I can’t swear that Khan mentioned the other thing that is most relevant about sars: It was caused by a novel coronavirus.
Ali Khan is now the dean of the College of Public Health at the University of Nebraska Medical Center, in Omaha. He seems an unlikely Omahan: born and raised in Brooklyn, by Pakistani immigrant parents, he went to Brooklyn College, followed by suny Downstate (in Brooklyn) for medical school. “And then I did this crazy thing of leaving Brooklyn”—crazy to his family, “because I have uncles and aunts who have never yet left Brooklyn to go to the city.” His father, Gulab Deen Khan, was a self-made man of the epic sort: as a teen-age peasant farmer, he trekked from Kashmir to Bombay, lied about his age, and got work on a ship, greasing engines. His friends called him Dini, as a diminutive, because he was small. After moving to the U.S., Dini Khan stoked coal in boilers to heat apartment buildings in Brooklyn until he had saved enough to buy an apartment building himself. He made money—what seemed a fortune. Before he lost it, in another speculation, Dini Khan decided that his young son, Ali, should learn about his family’s culture, religion, and language. He sent Ali back to Pakistan for middle and high school. By parental miscalculation, he chose a classic British boarding school in Lahore, a better place to learn cricket than Urdu or Islam. Ali Khan, now fifty-six years old, told me this story, punctuated with laughs, when I reached him recently by Skype. His dark hair and beard had grayed a bit, but he still looked fit and sounded jovial. He spoke of Omaha like a pitchman for the Chamber of Commerce: great city, safe, unpretentious ethos, full of billionaires, such as Warren Buffett, who live in their old family homes, drive their little Buicks, and write million-dollar checks to the community.
“I love being a dean,” he said. “It’s so much fun.” He went to Omaha in 2014, leaving the directorship of the C.D.C.’s Office of Public Health Preparedness and Response, which included overseeing the Strategic National Stockpile of emergency medical supplies, supervising eight hundred employees, helping assemble a national biodefense strategy against pandemic threats, and much else. “The end of my career at C.D.C., I managed a $1.5-billion budget, so it was people and money.” He had travelled the world on outbreak responses, from Wyoming to Bangladesh. During a mission to southern Chile, investigating a hantavirus outbreak, he visited remote villages, sometimes on horseback, trapping rodents to determine which species carried the virus. “We learned quickly that there were a lot of rodents,” he said. After he worked on Rift Valley fever in Saudi Arabia, in 2001, the Saudi Minister of Health gave him a Lucite replica of a beheading sword as a token of gratitude. At one dicey moment in central Zaire, during an outbreak of monkeypox, he and his team got word that two sets of combatants in the raging civil war—Laurent Kabila’s guerrillas and the opposing forces of President Mobutu—were coming. “They’ll likely take your vehicles and gear,” an American Embassy contact advised by satellite telephone. “But they probably won’t kill you.” Khan’s group packed fast and vamoosed on a small airplane, which rose straight into a thrashing thunderstorm. “The guy on my left was praying,” Khan recounted in a book, “The Next Pandemic,” full of colorful field adventures and serious warnings, published in 2016. “I looked over and saw that the French physician sitting next to me was writing a farewell note to his family. Which got me thinking.” His thought: This is a risky profession, and the work has to be worth a person’s life. For more than two decades at the C.D.C., it evidently was. In 1995, he did that hitch in Kikwit, Zaire, for Ebola. The following year, he went to the Sultanate of Oman to help with Crimean-Congo hemorrhagic fever. Uganda, in 2001, for Ebola again. sars, in Singapore, in 2003. Chad was still struggling to eliminate polio in 2008, and Khan went there.
But, toward the end of his tenure with the C.D.C., as a high-level bureaucrat, he was responsible for orchestrating, not investigating; science was a small slice of the job. “Now it’s almost all science,” he said. Virology, epidemiology, ecology, and other aspects of disease science provide the substance of his mission, “educating the next generation of public-health practitioners.”
The eclectic décor of his current office includes electron micrographs of various pathogens hung like portraits in a rogues’ gallery, two sculptures of mosquitoes as big as crows, a “Star Wars” clock, a “Big Hero 6” toy robot, cards sent from children all over the world, mementos and gifts from his travels—a Congolese incense burner, the Saudi beheading sword—and a whiteboard on which he records what he calls “my metrics.” His precious metrics: measures of progress toward academic goals for his school, scientific goals, philanthropic goals to support the work. “I’m evidence-based and evidence-driven,” he said.
I asked Khan about covid-19. What went so disastrously wrong? Where was the public-health preparedness that he had overseen at the C.D.C.? Why were most countries—and especially the U.S.—so unready? Was it a lack of scientific information, or a lack of money?
“This is about lack of imagination,” he said.
There were warnings. One of them was Khan’s favorite disease, sars. In late 2002, an “atypical pneumonia” of unknown origin began spreading in and near the city of Guangzhou, in southern China—one of the largest urban agglomerations on the planet. In January, 2003, in the body of a portly seafood merchant suffering a respiratory crisis, the virus reached a Guangzhou hospital. In that hospital, and then at a respiratory facility to which he was transferred, the man coughed, gasped, spewed, and sputtered during his intubation, infecting dozens of health-care workers. He became known among Guangzhou medical staff as the Poison King. In retrospect, disease scientists have applied a different label, calling him a super-spreader.
One infected physician, a nephrologist at the hospital, experienced flu-like symptoms but then, feeling better, took a three-hour bus ride to Hong Kong for his nephew’s wedding. Staying in Room 911 of the Metropole Hotel, the doctor became sick again, spreading the disease along the ninth-floor corridor. In the days that followed, other guests on the ninth floor flew home to Singapore and Toronto, taking the disease with them. Several weeks later, the World Health Organization called it sars. (The Metropole, having become notorious, was later renamed.) By March 15th, the W.H.O. was reporting a hundred and fifty new sars cases worldwide.
Two mysteries loomed, one urgent and one haunting: What was the cause—a new virus, and if so what kind?—and from what sort of animal had it come? The first mystery was soon solved by a team led by Malik Peiris, a Sri Lankan doctor who got a degree in microbiology at Oxford before going to the University of Hong Kong. Peiris specialized in influenza, and he suspected that H5N1, a flu virus that is troublesome in birds and often lethal in people but not infectious person-to-person, might have evolved into a form transmissible among humans. His team managed to isolate a new virus from two patients. It was a coronavirus, not a flu bug—that is, it was from a different virus family, with different familial traits. But the mere presence of this new virus in two sars patients did not mean that it was the cause of the disease. Then Peiris’s team showed with antibody testing that it might indeed be the sars agent, and further work proved that they were right. Although earlier tradition tended toward naming new viruses by geographical association—Ebola was a river, Marburg a city in Germany, Nipah a Malaysian village, Hendra an Australian suburb—greater sensitivity about stigmatization prevailed. The pathogen became known as sars-CoV. Recently, the name has been revised to sars-CoV-1, so that the agent of covid-19 can be called not Wuhan virus but sars-CoV-2.
SARS reached Toronto on February 23, 2003, carried by a seventy-eight-year-old woman, who, with her husband, had spent several nights of a two-week trip to Hong Kong on the ninth floor of the Metropole Hotel. The woman sickened, then died at home on March 5th, attended by family, including one of her sons, who soon showed symptoms himself. After a week of breathing difficulties, he went to an emergency room and there, without isolation, was given medication through a nebulizer, which turns liquid into mist, pushing it down a patient’s throat. “It helps open up your airways,” Khan told me—a useful and safe tool to prevent, say, an asthma attack. But, with a highly infectious virus, unwise. “When you breathe that back out, essentially you’re taking all the virus in your lungs and you’re breathing it back out into the air—in the E.R. where you’re being treated.” Two other patients in the E.R. were infected, one of whom soon went to a coronary-care unit with a heart attack. There he eventually infected eight nurses, one doctor, three other patients, two clerks, his own wife, and two technicians, among others. You could call him a super-spreader. One E.R. visit led to a hundred and twenty-eight cases among people associated with the hospital. Seventeen of them died.

In Singapore, the first sars case was a young woman who had also stayed at the Metropole, and had, on March 1st, sought help for fever, cough, and pneumonia at Tan Tock Seng Hospital, one of Singapore’s largest facilities. She had visitors, and, when several of them returned as patients, doctors suspected something contagious. Then four nurses from the young woman’s ward called in sick on one day, an abnormality noticed by Brenda Ang, a physician who was in charge of infection control at the hospital. “That was the defining moment for me,” Ang, a tiny, forthright woman, said, when I visited her at the hospital. “Everything was accelerating.” It was Thursday, March 12, 2003, the day that the W.H.O. issued a global alert about this “atypical pneumonia.”
At about that time, Ali Khan arrived in Singapore, serving as a W.H.O. consultant (seconded from the C.D.C.) to help organize an investigation and a response. He met daily with Suok-Kai Chew, the chief epidemiologist at the Ministry of Health, and along with others they developed strategy and tactics, getting governmental coöperation through a sars task force. The public-health strategy was isolation and quarantine. “Before this outbreak, quarantine and isolation were not often evoked for infectious-disease outbreaks,” Khan told me—at least, not in the recent past. During the medieval plagues in Europe, infected unfortunates were sometimes sent outside city walls, to die or recover; the Mediterranean seaport Ragusa (now Dubrovnik) established a trentino, a thirty-day quarantine for travellers arriving from plague zones. In late-nineteenth- and early-twentieth-century America, during smallpox outbreaks, victims showing pox (especially if they were poor people or people of color) could be confined in quarantine camps, surrounded by high fences of barbed wire, or in nightmarish “pesthouses”—not so much to be treated but for the safety of the general populace. “That was a concept that had sort of gone out of vogue,” Khan told me dryly. He and Chew and their colleagues revived it in a more humane version.
Tan Tock Seng started treating only sars patients, with other sick people diverted to Singapore General. Every suspected or probable case of sars went into isolation at T.T.S., and the definition of “suspected or probable” was expanded beyond W.H.O. guidelines to include anyone with a fever or respiratory trouble. All health-care workers suited up with personal protective equipment, including N95 masks, and they were required to check themselves for fever or other symptoms three times a day. Medical staff were also restricted to one institution, so they couldn’t carry the virus between hospitals. During risky procedures, such as intubating a patient, they wore respirator helmets that pumped in purified air.
Firm measures were also taken to limit the disease’s spread in the community. As of March 27th, schools closed, and the bodies of those who died of sarswere cremated within twenty-four hours. Investigators traced close contacts of each new sars patient, also within twenty-four hours, and those contacts were consigned to mandatory self-quarantine. “O.K., you are staying home. There will be a camera we’re setting up in your house, and there’s a phone,” Khan said, recounting the instructions. “We will call you randomly, and you’re expected to turn on the camera and be there.” Already, more than eight hundred people were quarantined. Flout the home quarantine, and you’d be tagged with an electronic tracer, such as an ankle bracelet. Mandatory quarantine brought logistical challenges, Khan told me: “ ‘The moment you hold ’em, you own ’em,’ is what we say.” You’ve got to feed these people, see to their health care, make sure they are housed and clothed. “Who takes care of them? Who pays for them?” If you’re the government ministry enforcing self-quarantine, you do.

By April 24th, twenty-two people had died, at which point penalties for quarantine-breakers stiffened: bigger fines, the possibility of jail. Taxi-drivers had their temperature checked daily. Passengers departing and arriving at Changi Airport were also screened, as well as people travelling in buses and private automobiles. On May 20th, eleven people were fined three hundred dollars each for spitting. These measures worked. On July 13, 2003, the last sarspatient walked out of Tan Tock Seng and it was over. Some people loosely say that sars“burned out,” having killed only seven hundred and seventy-four people worldwide. It didn’t burn out. As Ali Khan told me, it was stopped.
“What are you most concerned about now?” I asked Brenda Ang, at Tan Tock Seng, six years later.
She laughed in frustration. “Complacency,” she said. “And apathy.” Mundane but crucial infection-control measures—the assiduous hand washing and wiping of doorknobs with alcohol—can lapse after a crisis. “People become complacent. They think there is no new bugs around.” And larger lessons, beyond the outbreak locale, beyond Singapore? “There’s no point just protecting your own turf,” she said. “Infectious diseases are so globalized.”
Ali Khan later told me the same thing: “A disease anywhere is a disease everywhere.”
In 2015, a different coronavirus arrived in South Korea, in the body of a sixty-eight-year-old man returning from business on the Arabian Peninsula. Middle Eastern respiratory syndrome (mers) had been recognized as a disease three years earlier, and nicknamed camel flu, because dromedary camels seem to carry the virus and transmit it to people. The mers virus may have originally come from bats—the Egyptian tomb bat, perhaps—but has probably been circulating in camels for at least thirty years. It may have spilled over into humans earlier than 2012, but, if so, those infections went unnoticed. No one knows whether the Korean businessman was sneezed on by a camel sometime during his stops in Bahrain, Qatar, Saudi Arabia, and the United Arab Emirates, or whether he picked up his infection from a person, but that question probably mattered little to the hundred and eighty-six South Koreans who became infected from him, directly or indirectly, and still less to the thirty-eight who died.
Super-spreader events drove this outbreak, too, but it was exacerbated by aspects of South Korea’s health-care system. Because citizens receive cheap medical care through a national insurance plan, with few restrictions on which hospital they visit, people often shop for treatment. The businessman visited three different hospitals after he felt sick, and was finally admitted to a fourth, in Seoul, where he was given a diagnosis of mers. By that time, he had infected twenty-nine people, of whom two became super-spreaders themselves, accounting for ninety-seven more cases. There were sometimes four or more beds in a hospital room, and patients were allowed to receive visitors, which contributed to the spread, as did poor ventilation, poor infection control, and narrow criteria for quarantine, so that people who picked up the infection through casual contact were missed. “They recognized at that point what happens with a coronavirus that causes health-care-acquired infections within your community and hopscotches from hospital to hospital,” Khan said. mers in South Korea became a textbook example of blunders that led to “nosocomial spread,” the term for health-care-acquired infections. When covid-19 arrived, Khan said, “I guess maybe it was raw for them.”
SARS touched the U.S. only gently, producing twenty-seven probable cases and no deaths, most likely for reasons amounting to luck. mers seemed even less notable: two cases in 2014, both in health-care workers returning from stints in Saudi Arabia, with no secondary spread. The C.D.C. noticed, but scarcely anyone else did.
Other warnings came from scientists. In a series of obscure but important papers published in the past fifteen years—most with the word “bat” in the title and often with the name Zheng-Li Shi in the list of authors—researchers illuminated the connections among coronaviruses, bats, and people.
Zheng-Li Shi is a virologist in her fifties, educated in Wuhan and France, who runs a lab at the Wuhan Institute of Virology. She made her first bat-catching expedition into Chinese caves in 2004, and a year later helped lead a group of researchers who showed that the sars virus, discovered by Peiris to cause the syndrome in people, came to humans from bats. Before that, there had been a false lead pointing toward the masked palm civet—a wild carnivore, roughly resembling a badger, that is prized in the wild-animal food trade—and thousands of captive civets were promptly slaughtered. Then better data came from Shi’s group. In 2013, she co-wrote a paper casting light on how some bat-borne coronaviruses—but not others—succeed in infecting humans. Their spike proteins (the knobby projections that give each viral particle its corona-like appearance) bind well to receptors not just on bat cells but on certain cells in the human respiratory tract. It’s sort of a hook-and-latch relationship, and the latches, known as ace-2 receptors, allow viral penetration of the cell. Once inside, the viral genome commandeers some of the cell’s apparatus to make copies of itself, and the infection takes off.
Around that time, Shi and her team began focussing on a cave on the outskirts of Kunming, the capital of Yunnan Province, in an area famous for its picturesque karst formations. Sampling bodily fluids from bats that used the cave as a roost, the researchers found a great diversity of coronaviruses, including three carrying just the right equipment—spike proteins capable of seizing ace-2 receptors—for infecting humans. “This work,” they warned in a 2017 paper, “highlights the necessity of preparedness for future emergence of sars-like diseases.” One strain of coronavirus they found, in a horseshoe bat, later took the label RaTG13 (not an acronym but a code of convenience). It’s worth casting an eye on that ungainly label, because RaTG13 is the closest known relative of what we now call sars-CoV-2, with a 96.2-per-cent genome similarity, which, as coronaviruses go, makes it like a first cousin.
One of Shi’s co-authors on that paper was a longtime collaborator of hers named Peter Daszak, who is the president of EcoHealth Alliance, a nonprofit scientific group, based in New York, devoted to biological conservation and pandemic prevention. Daszak praises Shi for her tireless scientific diligence, the solidity of her lab work, and more. “I’ve been in the field with her, I’ve done karaoke with her,” he told me. “She’s the No. 1 singer at the Wuhan Institute of Virology.”
Shi and Daszak and their colleagues not only warned the world, three years ago, that a new sars-like disease was possible. They held up for inspection, as though with a pair of tongs, a close variant of the virus that would cause the covid-19 pandemic. (Questions were recently raised in the Washington Postabout the possibility that a virus grown in Shi’s lab might have escaped containment, seeding the Wuhan outbreak, but so far there’s no scientific evidence for that and considerable evidence against it.) Furthermore, they added, it wasn’t just one virus that we needed to be wary of, since various sars-like viruses capable of using the ace-2 receptor “are still circulating among bats in this region.”
The new virus revealed itself gradually in humans last December, in Wuhan, and in January several Chinese laboratories, Shi’s among them, sequenced wholly or partly the genomes of samples from different patients, including five complete genomes. Shi and her colleagues made their announcement, on January 23rd, that the virus found in those five patients was 96.2-per-cent identical to the bat coronavirus they had warned about three years earlier. By that time, the virus had been circulating in Wuhan for at least seven weeks, and three consequential misconceptions had been propagated, not just by political leaders but by hospital officials and the Chinese version of the C.D.C.: that the outbreak had begun in the Huanan Seafood Wholesale Market, which famously sold much more than seafood; that the virus wasn’t dangerous; and that it didn’t pass from person to person. On the second and third points, there was disagreement by clinicians treating patients, such as Zhang Li, at Wuhan’s Jinyintan Hospital, who told the Wall Street Journal in late February, “I was on alert because this was a new pneumonia and because I’d dealt with sars.”
The misconception that the market was the origin of the outbreak is implicitly contradicted by a scientific paper published in late January, by a group of physicians from Wuhan and Beijing, describing clinical features of the first forty-one patients. Twenty-seven of them, the paper said, had been exposed in the Huanan market. Since a single horseshoe bat would be unlikely to infect twenty-seven people, even if they diced it into hors d’œuvres, and since by some accounts bats weren’t even on sale in the market at that time, a few scientists have speculated that there was an intermediate host animal—a snake, a pangolin, a palm civet?—in which the virus amplified itself, before that larger creature was sold or butchered. The molecular evidence for snakes is weak, pangolins are a complicated story, and civets aren’t implicated this time. An American physician and scholar named Daniel R. Lucey (who had also worked the sars outbreak, in Guangzhou, Hong Kong, and Toronto) wondered about the fourteen other early patients. He noticed that the first of them, falling sick on December 1st, had no direct or secondary contact with the market. That meant, given the incubation period, that the virus must have been circulating in Wuhan outside the market since November. This doesn’t controvert the likelihood of the virus originating in a bat, but it suggests that perhaps it went into the Huanan market, as well as coming out of it, in humans. sars-CoV-2 is a subtle bug.
Singapore, with sars vivid in memory, reacted quickly and firmly to covid-19, closing the border to nonresidents, putting to use the isolation hospitals and negative-pressure rooms built since 2003, testing abundantly, tracing contacts and consigning them to home quarantine, and integrating political and health leadership to produce lucid, honest, consistent messaging. Despite all this, the country was not in lockdown until early April, when numbers shifted abruptly and a second wave struck.
South Korea, likewise, has used extensive testing, isolation, and quarantines to keep its caseload low. Although the capital, Seoul, is less than three hours from Wuhan by air, South Korea has had fewer cases and deaths than Sweden or Peru. Of course, that could change fast.
“South Korea is a good example for us to look at,” Khan told me. The first South Korean case was confirmed on January 20th, the same day as the first confirmed U.S. case. “They took a very different approach, and all we had to do was look at what they were doing and say, ‘We’re going to do the same thing.’ But we did not.” The first genome sequence of the virus from a human became available, from China, on January 10th. South Korean officials, after confirming their initial case, met promptly with medical-supply companies and urged them to develop test kits and start mass production. Scientists in the U.S. soon had their own sequenced samples, but time passed without meaningful action. “Every day after January 22nd was a day missed—by the U.S. government,” Khan told me. We could have called in Becton Dickinson (a giant medical-technology company) and told its leaders that we wanted nationwide testing capacity by the following Monday, he said. We didn’t. Why? Lack of imagination. Scientists could describe the risks, public-health officials could chart a response, but agency bureaucrats and national leadership failed to comprehend how bad the outbreak could be. On March 30th Donald Trump said, “Nobody had any idea.”
The first reported U.S. case involved a thirty-five-year-old man who had visited relatives in Wuhan before returning to the Seattle area on January 15th. (Lately, the news has broken of two other early cases, in Santa Clara County, California, that suggest the virus may have been present in the U.S. before January 15th; both patients died in February, but their covid-positive status was only detected, from autopsy evidence, in late April.) The Seattle-area man turned up at an urgent-care clinic on January 19th with complaints of a persistent cough and fever. His cough represented sars-CoV-2’s most obvious means of dispersing to other hosts, and so, for at least four days, this man could have passed the infection to others in Snohomish County, adjacent to Seattle, and possibly also on the airplane (if he was shedding virus though not yet symptomatic). At the clinic, his travel history raised concern, so an urgent-care provider notified personnel at the state health department, who notified the C.D.C.’s Emergency Operations Center. Get samples and we’ll test him, the C.D.C. said. The man gave blood and swab samples, then went home. The next day, when his test results were positive, he was admitted to a hospital and placed in an isolation unit.
The disastrously tardy, inadequate, confused, and (for many citizens) confusing response of the federal government to covid-19, both before and after the first case, derives from too many factors to list here, but I’ll mention two: failure to appreciate the sars and mers warnings, both delivered by other coronaviruses; and loss of capacity at high government levels, within recent years, to understand the gravity and immediacy of pandemic threats. The result of that loss is what Ali Khan means by lack of imagination. Beth Cameron, a former head of the Directorate for Global Health Security and Biodefense on the National Security Council staff, calls it the absence of “the smoke alarm.” Those in power who are charged with “keeping watch to get ahead of emergencies” need to smell the smoke and smother the fire while it’s small, Cameron told me. “You’re not going to stop outbreaks from happening. But you can stop outbreaks from becoming epidemics or pandemics.” She led the directorate from its establishment, following the 2014 Ebola epidemic in West Africa, until March, 2017. It survived under her successor for a little more than a year, and then, after John Bolton became the national-security adviser, it was dissolved. A smoke alarm doesn’t work when the battery has been removed.
Dennis Carroll, a former research virologist, led a pandemic-threats unit at the U.S. Agency for International Development for almost fifteen years. In 2009, he created a large program called predict, dispersing about two hundred million dollars in grants to support discovery of potentially dangerous new viruses before they spill over into humans. That program is ending, due to “the ascension of risk averse bureaucrats,” he told the Times, last October. He mentioned the White House closure of the N.S.C. health directorate as a parallel instance, and said that both Congress and the Administrations of George W. Bush and Barack Obama were “enormously supportive,” but then came the current chill winds.
The U.S. is not alone. “The global community has a really difficult time investing in what you think of as risk,” Carroll told me recently. Spending big money is itself a form of risk, especially if it’s public money, even if you’re spending it to insure against a greater risk. What if you spend a billion dollars, or ten billion—small change compared with what covid-19 is now costing—and the pandemic doesn’t occur during your term in office? “There’s very little appetite for that when the threat isn’t clear and present,” Carroll said. When sars happens, when a swine-flu pandemic happens, when an Ebola epidemic happens, political leaders and private donors react with fretful largesse, but when the crisis ends, he said, “we see a total collapse of those kinds of investments.” Homeowners buy fire insurance, governments buy vast armories of weaponry hoping they won’t be used, but there’s reluctance to invest seriously in preparedness against pandemics. “It’s attention-deficit disorder on a global scale,” Carroll said.
At the end of “The Next Pandemic,” Ali Khan offered another metaphor: “The time has come for us to move beyond seeing public health as the ax in the display case, where the sign says in case of emergency, break glass.” We need investment in preventive measures, he wrote, to make our communities resilient against such a nightmare—and that means viral discovery in the field; vigilant monitoring for spillovers; systems to produce diagnostic tests fast and in great abundance; better surge capacity of health-care providers; smart supply chains for P.P.E. and ventilators, and coördinated plans for moving them from one jurisdiction to another; coördinated planning among cities, states, provinces, nations, and international agencies for containing infectious disaster; public education to stiffen willingness to endure social distancing and quarantine monitoring; better public-health leadership and reliable funding cycles; and, most critically, the political will to risk paying for preparedness that might not be needed.
Maybe we will have those for the next pandemic, but it’s too late for vigilant preparedness against this one. “Usually, my personal role is to respond to these outbreaks overseas,” Khan told me the last time we Skyped. Such missions have spanned his C.D.C. career and beyond. But this time he hasn’t travelled. “There’s more than enough work right here in America,” he said. He might spend part of a day on decisions about fall classes and budget shortfalls at the College of Public Health, working to move convocation online, consulting with state or local officials about public-health measures or with private companies about keeping their employees and customers safe. When fifty-seven Americans who had been evacuated from Wuhan landed at the Omaha airport, in early February, Khan helped arrange for their quarantine at Camp Ashland, a National Guard base along the Platte River. He does media interviews, oversees the faculty deploying student teams for contact tracing in Nebraska and Iowa, advises on improvements to meat-packing facilities, and serves on the steering committee of the Global Outbreak Alert and Response Network, a linkage of experts working under the W.H.O. to study, anticipate, and respond to disease events. Like most of us now, he spends much of his time on Skype, Zoom, and the telephone, but for him the substance of discussions runs to drug-trials research, immune response, the latest in disease modelling, and how best to decontaminate N95 masks.
The case count for Nebraska is rising, from one confirmed patient, on March 6th, into the thousands. The state ranks low in cases and deaths, but also low in testing, so the real number of infected Nebraskans is unknown. Governor Pete Ricketts has closed schools, forbidden gatherings of more than ten people in some counties, and declared a state of emergency, but has declined to issue a stay-at-home order. Omaha is the county seat of Douglas County, the state’s most populous, which has its busiest airport and has been hit with a significant number of cases. And so, as Ali Khan sits in his office, amid pictures and mementos from a life of charging to the front against infectious disease, the pandemic is coming to him.
